What is a stress fracture?
A stress fracture is a term used to describe a range of conditions from swelling within the bone, also known as a stress reaction, to a break (fracture) of the bone.
Healthy bones are in a constant state of remodelling and repair in response to normal activity. If “too much” stress is put on a bone then a stress reaction can occur. If this stress is not reduced then it may develop into a stress fracture.
Stress fractures most commonly occur in the lower limbs in children who are involved in sports that involve running and jumping. They usually occur when there is a sudden increase in training demand, such as training more frequently, for increased time, or increased intensity.
This increase in training puts outpaces bones ability to accommodate for the intensity of the higher level of activity.
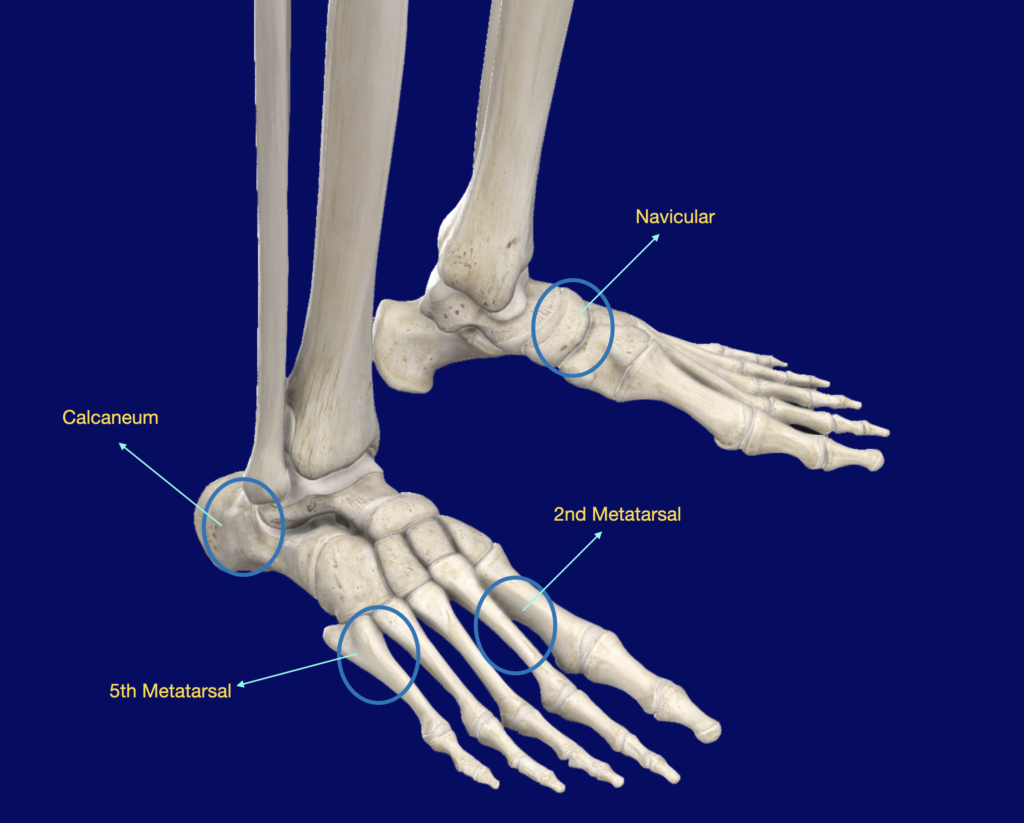
Stress fractures most commonly occur in the lower limbs, affecting the shin (tibia and fibula) and feet (metatarsal, navicular and calcaneus).
Who is most at risk of getting a stress fracture?
Factors such as being female, having a lower than normal Body Mass Index (BMI), abnormal periods and low bone density can put children and adolescents more at risk of developing a stress reaction. Tight muscles, particularly calf muscles, reduces the ability to absorb forces when running and jumping and can also put children at risk of a stress reaction.
Lockdowns with reduced activity has meant that children may have become less resilient to activity. Lack of sunlight and diet changes has made Vitamin D deficiency more common reducing bones strength and ability to remodel.

How does a stress fracture present?
Children with a stress fracture will usually experience pain with activity that builds as the activity continues. The pain will usually ease with rest. Swelling and tenderness may also be present at the site of a stress fracture.
How is a stress fracture diagnosed?
A stress fracture is diagnosed after considering a patients history (for example activity level/ training schedule and pain history) and clinical findings.
Plain radiology is important to rule out other causes, check alignment and may show established bony changes consistent with overactivity
In some cases imaging such as a bone scan or MRI may be indicated and the Vitamin D level checked.
What is the management for a stress reaction or stress fracture?
A complete history and examination is required to identify risk factors for stress fractures and evaluate lower limb alignment, foot posture and flexibility. Appropriate investigations performed and the diagnosis made excluding other causes of leg and foot pain.
A careful and gradual rehabilitation program will be prescribed. Your child must be pain free to progress throughout each phase of the rehabilitation program.
Sites for stress fractures in the foot
TREATMENT PLAN
Phase 1
Approximately Week 0 to 2
If your child experiences pain with walking, initial management will be immobilisation in a fibreglass cast or a special boot. Your child will need to use crutches to reduce weight bearing forces through the lower limb and stop all aggravating activities.
Phase 2
Approximately Week 2 to 4
Once your child can walk in a cast/special boot without pain they can progress into a shoe such as a sneaker/running shoe and gradually wean off crutches. Children can begin activity such as exercise in water, cycling and elliptical trainer to maintain strength and fitness. The key to recovery is reduced load bearing and not experiencing pain with activity.
Phase 3
Approximately Week 4 to 6
This phase of rehabilitation involves a very careful and gradual return to sport specific activities like training drills, but not competitive sport. Activity should be performed at a lower intensity than normal and gradually increased to make sure there is no recurrence of pain and allow the natural bony remodelling process to occur.
Phase 4
From Week 6
Gradual and careful return to sport.
If your child has remained pain free after two weeks of sport specific training drills then they can return to playing competitive sport.
If your child experiences any discomfort when progressing through this rehabilitation plan they will need to return to the previous phase of rehabilitation and not progress until they are pain free.