Paediatric Fractures
Fractures in children and adolescents are very different to those experienced by adults. Growth and development change the very nature of the types of fractures and injuries experienced and the treatment needs to include an appreciation of remodelling potential and a detailed knowledge of growth plate anatomy, function and management.
Paediatric Orthopaedic surgeons are expert in this respect and have techniques available to them that are not part of adult fracture management.
To better understand these differences the information presented gives an overview of paediatric fracture management
Anatomic differences: child to adult
The long bone in a child is divided into four regions: the diaphysis (shaft or primary ossification centre), metaphysis (where the bone flares), physis (or growth plate) and the epiphysis (secondary ossification centre).
In the adult, only the metaphysis and diaphysis are present
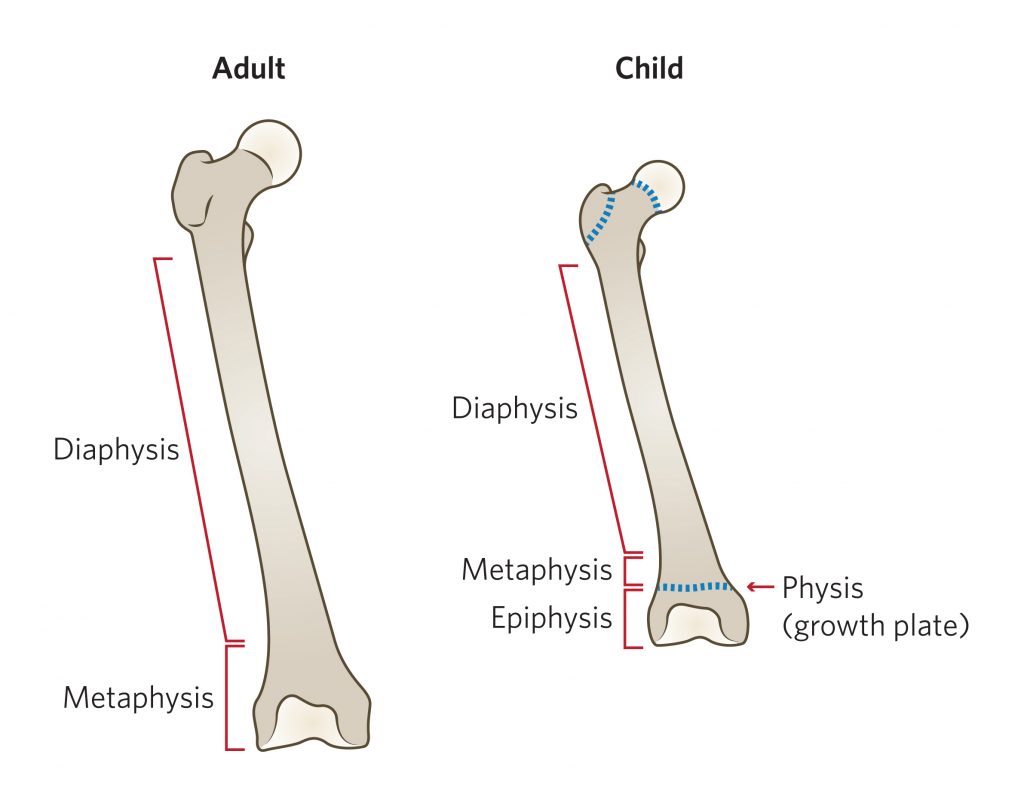

The epiphysis is completely or mostly cartilaginous in infants.
Initially it consists of articular cartilage and growth cartilage until these become differentiated by the development of a secondary ossification centre
The physis is responsible for the longitudinal growth of long bones whilst circumferential growth is mainly due to periosteal (appositional) growth.
Endosteal reabsorption is part of the growth/remodelling process but it’s counterintuitive to say that reabsorption contributes to growth.
The physis is a barrier to blood flow which may be critical during healing after physeal separations. Understanding which physes, are subject to complete disruption of the blood supply at the time of separation is a guide to the risk of long-term complications such as avascular necrosis (e.g. slipped upper femoral epiphysis).
Biomechanical differences between adult and child: Why do children’s bones bend before they break?
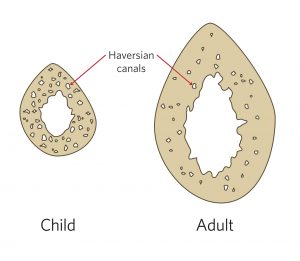
The osteoid density of a child’s bone is less than an adult’s. Juvenile bone is more porous than adult bone because the Haversian canals occupy a much greater part of the bone. This is the principal reason a child’s bone can bend more than an adult’s bone.
The ability to bend before breaking leads to unique fracture patterns in children including:
Buckle Injury: Failure of a child’s bone in compression results in a “buckle’ injury”, also known as a “torus” injury. These most commonly occur in the distal metaphysis, where porosity is greatest.

Plastic bowing (or deformation): Long bones may bend without breaking the cortex. Children’s bones can be bent to 45 degrees before the cortex is disrupted and a greenstick or a complete fracture occurs. However if the bending force is released the bone may only partially return to its pre-bent position, resulting in plastic bowing. The bones most commonly affected by plastic bowing are the ulna and fibula. In the ulna, plastic bowing may indicate a Monteggia fracture-dislocation. Because there is no obvious fracture of the ulna, the injury is frequently not diagnosed, resulting in delayed diagnosis and long-term morbidity

Greenstick fracture: A greenstick fracture occurs when there is sufficient energy to start a fracture but insufficient energy to complete it. The cortex fails on the tension side and the cortex on the compression side bends but remains intact. The degree of deformity is variable and sometimes complete reduction can only be achieved by deliberately completing the fracture i.e. fracturing the concave cortex, which is bent but not broken

Complete fractures: In children, the outer layer surrounding the bone, the periosteum, is much stronger than in adults but is loosely attached. Muscles arise from, and are inserted onto, the periosteum rather than the bone itself and this permits coordinated growth of the bone and the soft tissues. Complete fractures are rarely comminuted in children and are often less severely displaced than in adults. The periosteum is usually torn on the convex side of a fracture but the periosteum on the concave (compression) side may remain intact. The intact periosteum is able to act as a hinge, which restricts the degree of displacement and provides the key to closed reduction and position of immobilisation in a cast.

Physiological differences between adult and child: growth and healing
Due to the presence of growth plates, the healing of fractures in children is often much faster than in adults and is followed by a process of fracture remodelling. Factors affecting the remodelling capacity include:
Age: The rate of remodelling in a child is inversely related to age . In younger children remodelling is rapid and often complete. It is slower in older children and much slower in adolescents. A key is the number of years of growth remaining, from the time of injury to physeal closure. On average, physeal closure occurs in boys at age 16 and in girls at age 14 but there is a wide variation around these means. It is sometimes wise to formally check the bone age from a radiograph of the wrist or elbow than to rely on chronological age

Fracture site: Fractures close to the ends of long bones remodel much faster than those in the mid shaft. Therefore physeal injuries remodel faster than metaphyseal injuries, which in turn remodel faster than diaphyseal injuries. But there is also an influence on which end of the long bone is injured. The different rates of remodelling follow the rate of growth at the ends of the bone. In the upper limb, the most active growth plates contributing to longitudinal growth are those of the proximal humerus and distal radius and ulna . Hence, injuries of the proximal humerus and fractures close to the wrist remodel much faster than injuries of the elbow and proximal forearm. The reverse is true in the lower limb. Remodelling is fastest at the knee (distal femur and proximal tibia) than in the proximal femur and distal tibia
Relationship to joints: Remodelling is maximal in proximity to, and in the plane of action of, the nearest joint. The shoulder is a ball and socket joint; it moves in three planes and remodels in three planes. At least 30 degrees of angulation (in any direction) is acceptable in a child with more than two years of growth remaining. This is in contrast with fractures near the elbow, which is a hinge joint. Sagittal plane displacement remodels slightly but very slowly. Coronal plane displacement does not remodel at all. The cubitus varus or “gunstock” deformity after supracondylar fracture must be prevented because it will not remodel
Fracture healing
Fracture healing in children follows the same stages as that of adults but occurs at a much faster rate. Fractures heal by forming callus, which follows three overlapping phases: inflammatory, reparative and remodelling.
- Inflammatory phase (duration: hours–days): Broken bones result in torn blood vessels and the formation of a blood clot or haematoma. The inflammatory reaction results in the release of cytokines, growth factors and prostaglandins, all of which are important in healing. The fracture haematoma becomes organised and is then infiltrated by fibrovascular tissue, which forms a matrix for bone formation and primary callus.
- Reparative phase (duration: days–weeks): A thick mass of callus forms around the bone ends, from the fracture haematoma. Bone-forming cells are recruited from several sources to form new bone, which can be seen on radiographs within 7–10 days after injury (Figure 9). Soft callus is organised and remodelled into hard callus over several weeks. Soft callus is plastic and can easily deform or bend if the fracture is not adequately supported. Hard callus is weaker than normal bone but is better able to withstand external forces and equates to the stage of “clinical union”, i.e. the fracture is not tender to palpation or with movement.

- Remodelling phase (duration: months–years): This is the longest phase and may last for several years. During remodelling, the healed fracture and surrounding callus responds to activity, external forces, functional demands and growth. Bone (external callus) which is no longer needed is removed and the fracture site is smoothed and sculpted until it looks much more normal on an x-ray (Figure 9). The epiphyses gradually realign and residual angulation may be slowly corrected, in accordance with the rules of remodelling, outlined above
Growth Plate Anatomy
The growth plate, or physis, is the translucent, cartilaginous disc separating the epiphysis from the metaphysis and is responsible for longitudinal growth of long bones.
The cells of the physis are arranged in columns or layers described as the germinal or resting layer, the proliferative zone, the hypertrophic zone and the zone of provisional calcification (Figure 10). The proliferative zone is where the chondrocytes undergo rapid division by mitosis and is the most metabolically active zone. Osteoblasts use the chondrocyte columns as a scaffold for ossification in the zone of provisional calcification. The hypertrophic zone is the weakest because it lacks both collagen and calcified tissue. Most physeal separations occur through this layer because it is less able to resist shearing stress.

The macroscopic structure of the growth plates varies according to the degree of stress to which it is exposed. Around the knee, the stresses are high and in order to resist shear, the physis interdigitates with surrounding bone in what are known as mammillary bodies. This anatomic arrangement locks the physis solidly. If it does sustain a shear injury there is a higher chance of developing a bony bar across the physis and subsequent growth arrest. This is in contrast to the commonly injured distal radial physis that is more linear and rarely arrests.
Salter-Harris classification of physeal injuries
Although there are more recent and more complex classifications, the Salter-Harris classification is the most widely used and clinically useful approach to classifying and describing physeal injuries in children. About 90% of children with physeal injuries can be classified using the five Salter-Harris classifications from plain x-rays (Table 1). Another 5% can be classified using one of the more elaborate systems and the final 5% defy classification. When an apparently “unclassifiable pattern” is encountered, additional imaging may be helpful, including oblique views, an arthrogram, CT or MRI.
Type 1
Transverse fracture through the growth plate. Accounts for 6% of all physeal injuries

Type 2
Transverse fracture through the growth plate and an oblique or vertical fracture through the metaphysis. Most common type and accounts for 75% of all physeal injuries

Type 3
Transverse fracture through the growth plate and a vertical fracture through the epiphysis. Accounts for 8% of all physeal injuries

Type 4
Vertical fracture through all three components, metaphysis, physis and epiphysis. Accounts for 10% of all physeal injuries

Type 5
Compression fracture or crushing of the growth plate. This injury is rare and difficult to see on x-ray

The management of physeal injuries depends on the type of fracture pattern, bone involved and the amount of growth remaining. In general anatomic reduction performed as gently as possible will give the physis the best chance to recover and continue normal growth.
Sometimes an open procedure is better than a closed reduction but in any event careful technique is imperative and appropriate long term follow-up require to ensure that a growth disturbance does not occur.
Types of growth disturbances
- Complete Growth arrest – the injury to the growth plate is so severe that a complete fusion occurs and further growth does not occur (shortening)
- Part Growth arrest – the injury produces a partial arrest that with subsequent growth the tether inhibits part of the growth plate and causes a disturbance to longitudinal growth (shortening) or angulation (deformity)
Fracture Management principles
Analgesia first
Early immobilisation by temporary splinting, combined with reassurance can be very effective analgesia. Pain relief can be provided by paracetamol (20 mg/kg per dose) or diclofenac (up to 1 mg/kg per dose). Non-steroidal anti-inflammatory agents are especially useful for musculoskeletal pain. Procedural analgesia is very important in the ED and can be provided by many different means according to the child’s needs and the clinical setting. All forms of analgesia and sedation have specific risks and benefits. Most units have clinical practice guidelines to ensure safe and effective practice. Bier’s block is very useful for many forearm and wrist fractures. Entonox is also useful for simple fracture manipulations and reductions. Local anaesthetic blocks can also be useful, especially femoral nerve blocks for fractures of the femoral shaft.
Reassurance and education
No matter how trivial the injury, parents deserve an adequate explanation, appropriate advice and answers to their questions. Sometimes specific treatment is not required. Some minor buckle injuries may not require casting or immobilisation.
Simple splintage
When a fracture is undisplaced or minimally displaced, reduction may not be necessary. However, the majority of fractures and epiphyseal injuries are painful and immobilisation is often the best analgesic. Removable forearm splints are ideal as primary management for undisplaced fractures of the distal radius. A plaster backslab does not make a buckle injury heal more quickly but it does provide excellent pain relief. Splints for these injuries should be simple and safe and easy to put on and take off. A plaster backslab, held in place with a crepe bandage can be removed by parents or at the time of review by the child’s GP. Most complete plaster casts need to be removed in the ED or fracture clinic.
The simple formula, believed by many that “bony injury = a plaster cast” and “soft tissue injury = a bandage” is not always true. Some upper limb fractures are best managed in a collar and cuff or triangular sling. This includes most clavicle fractures and some proximal humeral fractures. Some soft tissue injuries in the lower limb, such as ankle sprains are more effectively managed in casts than with strapping because children can then weight bear with comfort and without the need for crutches. It is easier to go back to school walking in a below knee cast than trying to maintain partial weight bearing with crutches and ankle strapping.


Closed reduction and casting
Closed reduction and cast immobilisation is the treatment of choice for the majority of displaced fractures in children of all ages. Reduction is carried out under sedation, local anaesthetic block or general anaesthesia. The method of reduction varies according to the fracture type, direction and degree of displacement. The direction of fracture displacement is defined from x-rays and most reduction manoeuvres are based on reversing the forces that caused the fracture to displace. The position in cast, the type of cast and the duration of immobilisation depends on the fracture and the age of the child.
Plaster casts
The most commonly used means of maintaining reduction is plaster of Paris. Plaster casts can be safe, effective and cheap. However, there are risks and casts can inflict more serious damage than the presenting injury. “Plaster can be a disaster!” Care must be taken.
Backslabs
The backslab is the simplest and safest form of plaster splint. Instead of using encircling bandages, the plaster slabs are applied longitudinally to the limb and bandaged in place while still soft. As the plaster firms up, the slabs conform to the contours of the limb to provide support with less risk of limb constriction than with a complete cast.
Indications for backslabs include:
- Buckle injuries and minor physeal injuries at the wrist
- Most elbow fractures . Complete casts are not necessary and are dangerous, even if split
- Temporary support for many hand and foot injuries
- Tibial fractures with significant swelling
- Crush injuries and open fractures

Complete casts
The complete cast is not easy to apply in an effective, comfortable, and safe manner. Staff should be trained and aware of the potential for cast complications. Padding used should be adequate for skin protection and comfort without being so excessive as to permit movement. Casts are seldom applied by simply winding the plaster bandages around the limb. They are constructed from a mixture of plaster slabs and plaster bandages, applied together for both strength and lightness. The extremity should be appropriately positioned for comfort and safety and to minimise the risk of fracture re-displacement.
Most distal radial fractures are displaced dorsally. After reduction, the wrist is flexed and the position held by dorsal moulding of the cast, at the level of the fracture. The plaster is moulded by applying gentle pressure with the heel of the hands (not the fingers or thumbs) to the cast over the dorsal aspect of the wrist.


Further Information
Live links coming soon …